Bow legs & knock knees are the opposite deformity in the lower limb. In the bow leg, the leg is bowed outward from the knee and below so that the distance between the knees is high, but the ankle touches together, in the knock knee, both side of the knee on the medial surface touches together, but the distance between the ankles remains high. Both of these deformities can be physiological (a normal, natural occurrence) but also be because of some pathological ailment. Normally at the time of birth, most of the leg in a newborn is bowed outward, and slowly it corrects spontaneously around the age of 18 months to 2 years than in the natural course legs go in and develop a knock knee and become more prominent at the age of 3 years. Afterward, again they start correcting as natural progress and take the natural adult pattern of 5-7 degree Valgoid knee. That remains with the life of a person. If this variation in limb alignment persists beyond the age limit and of a high grade of deformity, then we need to identify the cause and treat it.
Other Causes of Bow Leg in children:
Ricket in children (Vitamin D Deficiency)
Skeletal dysplasia (abnormal bone development)
Blount disease
Achondroplasia
Growth plate injury
Other Causes of Knock Knee in Children:
Ricket
Skeletal dysplasia
Growth plate injury
Normally infant’s legs are bowed but if it looks beyond normal then parents should consult a pediatric orthopedic surgeon in india or pediatrician. We need to have a close watch on the progress of bowing. If the knock knee persists beyond 7-year age the parents also need to consult a specialist.
Symptoms:
Parents can easily recognize the bowing as well as knock knees just by looking at the leg without clothes. In the bowleg, the tibia is bent outward so that the space between the knees is more compared to the space in normal children. In knock knee, it is reversed. In this condition, both side knees touch each other in a standing position.
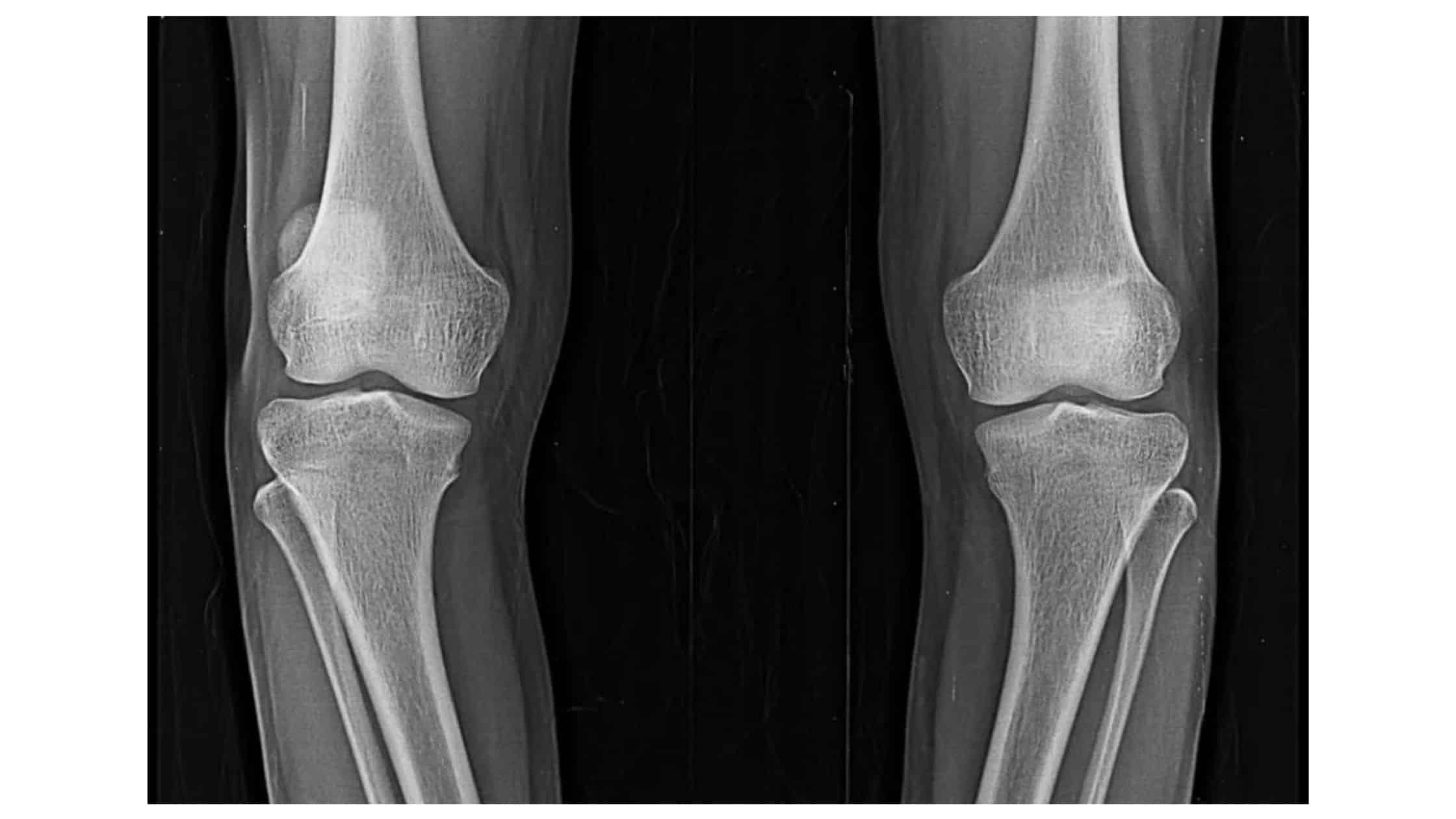
Diagnosis:
Primary diagnosis can easily be made just but examination of the child in a standing position & exposed both lower limbs. The first investigation is an x-ray if it is needed. In X-ray, we can determine the etiology. X-ray anteroposterior view of the lower extremity is required which should be taken in a standing position. It will give a clear diagnosis and severity of the deformity. Blood tests are required to see the level of Vitamin D.
Treatment:
Physiological variety of both bow leg and knock knee treatment doesn’t need any treatment except assurance to parents. If the bowing is more and occurs because of vitamin D Deficiency, then do you need vitamin D and calcium supplements? Usually, this bowing & knock knee correct spontaneously if dx in the early age group. Sometimes deformity is severe but bones are soft then a plaster or mermaid brace should be given to the child.
When the deformity is severe and the age is beyond 7 years in knock knee or 3 years in the bowing of the tibia then the child needs surgery to correct the deformity. The pediatric orthopedic surgeon will do surgery after evaluation. If the child has sufficient growth with him then the doctor will modulate physical plate growth by 8 plates or screws and if the child is crossed their growing age then cutting of the bone and correcting the deformity at once.
Blount disease requires special consideration in treatment planning but beyond discussion at this place.
For More Information: Pediatric Orthopedic Treatment FAQs
Reference link –
https://www.healthline.com/health/genu-valgum